16.3 Viral Infections of the Skin and Eyes
Learning Objectives
- Identify the most common viruses associated with infections of the skin and eyes
- Compare the major characteristics of specific viral diseases affecting the skin and eyes
Until recently, it was thought that the normal microbiota of the body consisted primarily of bacteria and some fungi. However, in addition to bacteria, the skin is colonized by viruses, and recent studies suggest that Papillomaviridae, Polyomaviridae and Circoviridae also contribute to the normal skin microbiota. However, some viruses associated with skin are pathogenic, and these viruses can cause diseases with a wide variety of presentations.
Numerous types of viral infections cause rashes or lesions on the skin; however, in many cases these skin conditions result from infections that originate in other body systems. In this chapter, we will limit the discussion to viral skin infections that use the skin as a portal of entry. Later chapters will discuss viral infections such as chickenpox, measles, and rubella—diseases that cause skin rashes but invade the body through portals of entry other than the skin.
Papillomas
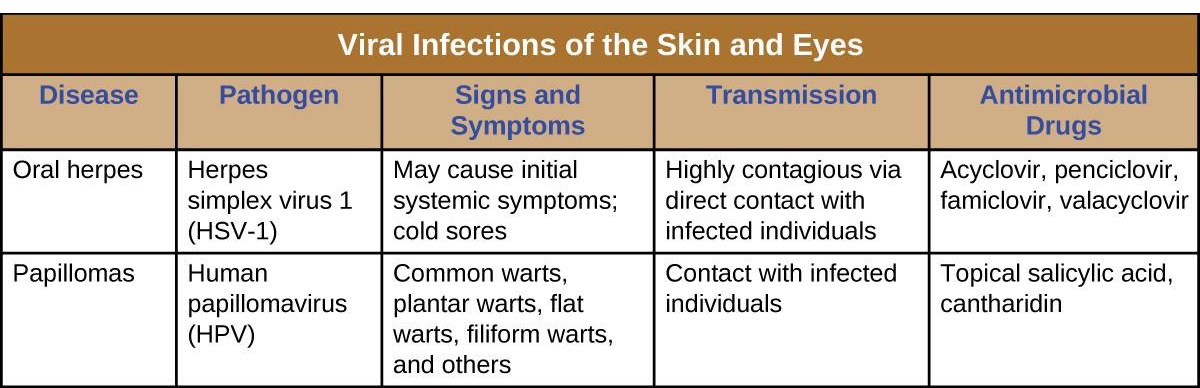
Papillomas (warts) are the expression of common skin infections by human papillomavirus (HPV) and are transmitted by direct contact. There are many types of HPV, and they lead to a variety of different presentations, such as common warts, plantar warts, flat warts, and filiform warts. HPV can also cause sexually-transmitted genital warts, which will be discussed in Urogenital System Infections. Vaccination is available for some strains of HPV.
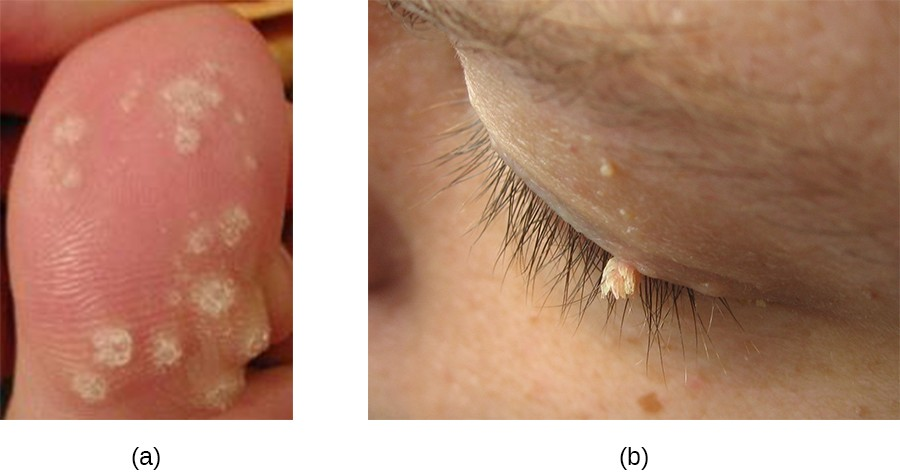
Common warts tend to develop on fingers, the backs of hands, and around nails in areas with broken skin. In contrast, plantar warts (also called foot warts) develop on the sole of the foot and can grow inwards, causing pain and pressure during walking. Flat warts can develop anywhere on the body, are often numerous, and are relatively smooth and small compared with other wart types. Filiform warts are long, threadlike warts that grow quickly.
In some cases, the immune system may be strong enough to prevent warts from forming or to eradicate established warts. However, treatment of established warts is typically required. There are many available treatments for warts, and their effectiveness varies. Common warts can be frozen off with liquid nitrogen. Topical applications of salicylic acid may also be effective. Other options are electrosurgery (burning), curettage (cutting), excision, painting with cantharidin (which causes the wart to die so it can more easily be removed), laser treatments, treatment with bleomycin, chemical peels, and immunotherapy (Figure 16.19).
Oral Herpes
Another common skin virus is herpes simplex virus (HSV). HSV has historically been divided into two types, HSV-1 and HSV-2. HSV-1 is typically transmitted by direct oral contact between individuals, and is usually associated with oral herpes. HSV-2 is usually transmitted sexually and is typically associated with genital herpes. However, both HSV-1 and HSV-2 are capable of infecting any mucous membrane, and the incidence of genital HSV-1 and oral HSV-2 infections has been increasing in recent years. In this chapter, we will limit our discussion to infections caused by HSV-1; HSV-2 and genital herpes will be discussed in Urogenital System Infections.
Infection by HSV-1 commonly manifests as cold sores or fever blisters, usually on or around the lips (Figure 16.20). HSV-1 is highly contagious, with some studies suggesting that up to 65% of the US population is infected; however, many infected individuals are asymptomatic.[1] Moreover, the virus can be latent for long periods, residing in the trigeminal nerve ganglia between recurring bouts of symptoms. Recurrence can be triggered by stress or environmental conditions (systemic or affecting the skin). When lesions are present, they may blister, break open, and crust. The virus can be spread through direct contact, even when a patient is asymptomatic.
While the lips, mouth, and face are the most common sites for HSV-1 infections, lesions can spread to other areas of the body. Wrestlers and other athletes involved in contact sports may develop lesions on the neck, shoulders, and trunk. This condition is often called herpes gladiatorum. Herpes lesions that develop on the fingers are often called herpetic whitlow.
HSV-1 infections are commonly diagnosed from their appearance, although laboratory testing can confirm the diagnosis. There is no cure, but antiviral medications such as acyclovir, penciclovir, famciclovir, and valacyclovir are used to reduce symptoms and risk of transmission. Topical medications, such as creams with n-docosanol and penciclovir, can also be used to reduce symptoms such as itching, burning, and tingling.

![]()
- What are the most common sites for the appearance of herpetic lesions?
- Wald, A., and Corey, L. “Persistence in the Population: Epidemiology, Transmission.” In: A. Arvin, G. Campadelli-Fiume, E. Mocarski et al. Human Herpesviruses: Biology, Therapy, and Immunoprophylaxis. Cambridge: Cambridge University Press, 2007. http://www.ncbi.nlm.nih.gov/books/NBK47447/. Accessed Sept 14, 2016. ↵
